![]()
Low homocysteine occurs when homocysteine in the bloodstream drops below healthy ranges. This can impact methylation, detoxification, neurotransmitters, and energy production.
Low Homocysteine Levels: What are The Consequences?
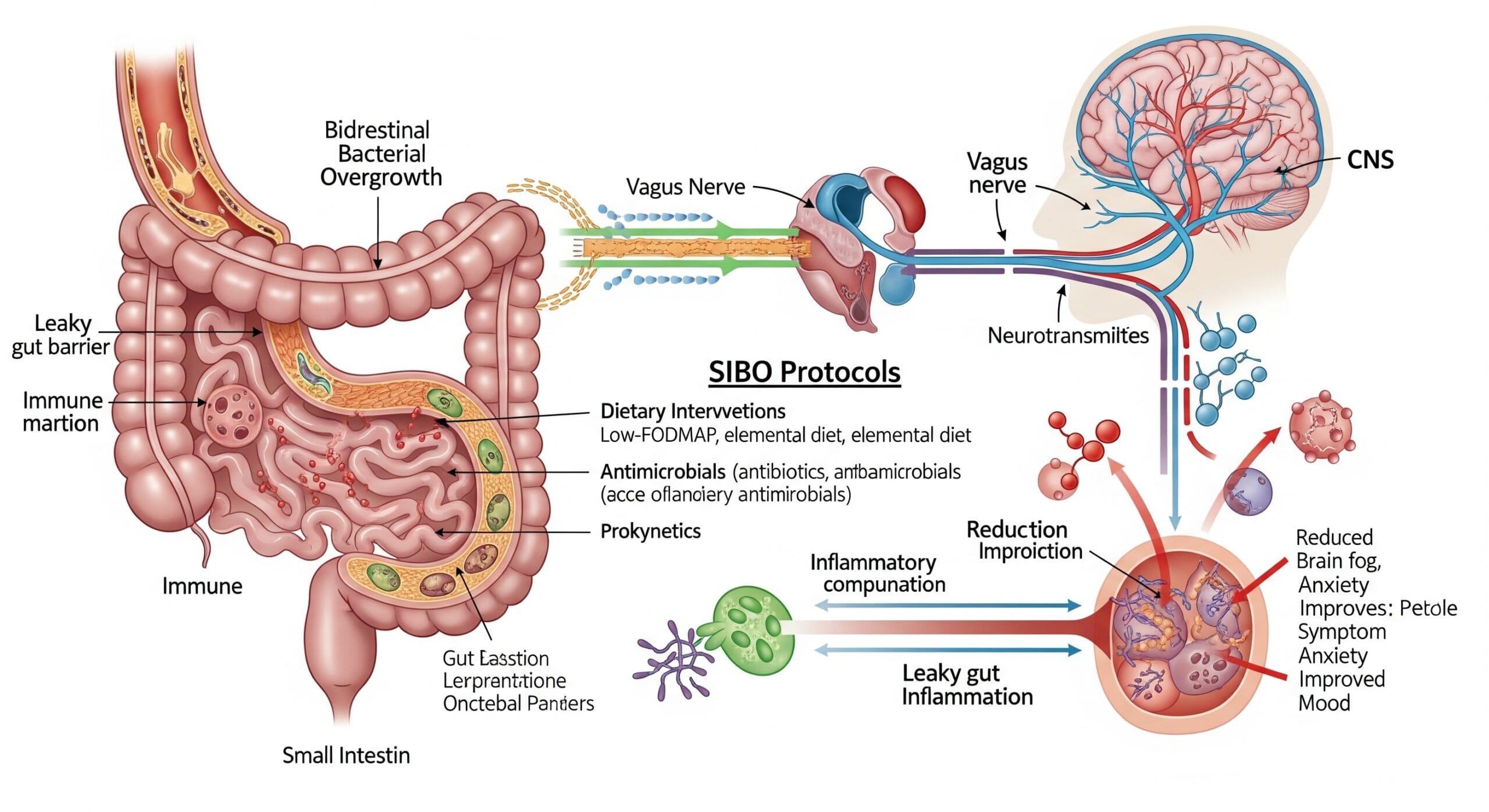
Homocysteine is an amino acid derivative that serves as an intermediate in the synthesis of methionine and cysteine. It contains a sulfhydryl group that serves as an important branch in the formation of important biological compounds such as glutathione (GSH) and S-adenosylmethionine (SAM). GSH is formed through the transsulfuration (TS) pathway with the formation of cysteine from homocysteine by a stepwise process by the enzymes cystathionine-beta-synthase (CBS) and cystathionine-gamma-lyase (CGL), and by subsequent formation of GSH by glutathione synthetase. SAM is formed by methylation of homocysteine to form methionine by the enzyme N5,N10-methylenetetrahydrofolate reductase (MTHFR) and subsequent condensation of methionine with adenosine triphosphate (ATP) to form SAM.
Low homocysteine levels, or hypohomocysteinemia, is the result of several factors. It can be a result of a metabolic insult which prompts the body to produce more GSH than normal, low intake of the amino acids methionine and cysteine (methionine predominantly comes from meat protein so those that don’t eat meat or eat too little may be at higher risk), an inherently low level of the enzyme MTHFR, low intake of vitamins folate and B12, or increased detoxification of xenobiotics through the phase II liver reaction sulfation. These factors will result in low homocysteine levels, which would then lead to a variety of clinical disorders.
Hypohomocysteinemia has been shown to play a role in the malnutrition-inflammation-cachexia syndrome with which low dietary intake of methionine would lead to worsening of chronic kidney disease, with which homocysteine can be a variable in determining survivability of the patient. Hypohomocysteinemia is also a cause of the progression of atherosclerosis in cardiovascular diseases.
Since hypohomocysteinemia may also present with a lack of cysteine levels, it can be due to the role that the liver plays. Synthesis of GSH requires cysteine, in which the formation of GSH will get homocysteine from the reservoir to support the body in times of oxidative stress, in which GSH may be able to mediate and prevent oxidative damage to cells. The synthesis of GSH would therefore favor the TS pathway. So basically this means if there is a low level of antioxidants, the body will steal cysteine from homocysteine to support glutathione production. So low homocysteine may be a sign of oxidative stress.Formation of more cysteine from homocysteine would then deplete the homocysteine pool to support the formation of GSH to combat the free radicals.
Another factor that would deplete homocysteine levels would be the detoxification pathway sulfation. Sulfation is a phase II or conjugation reaction in which cysteine donates a sulfur group to the xenobiotic forming a xenobiotic-sulfate, allowing it to be excreted from the system. Apart from sulfation, cysteine is also employed in the formation of bile acids such as taurine. Taurine is especially synthesized when the body takes in fat and alcohol. Synthesis of taurine would also deplete homocysteine levels by promoting the TS pathway in the formation of cysteine. These homocysteine-depleting mechanisms are prevented if there are adequate amounts of methionine and cysteine from the diet.
Low dietary intake of vitamins folate and B12 can also lead to hypohomocysteinemia. Folate is an important component of the methylation pathway as it forms the structure of N5,N10-methylenetetrahydrofolate and would therefore be an important substrate for the transmethylation pathway involving the formation of SAM by transferring a methyl group from N5,N10-methylenetetrahydrofolate to homocysteine forming methionine, catalyzed by the enzyme MTHFR. Folate is important in regulating gene expression by regulating levels of SAM.3
Vitamin B12 is another vitamin that is important in gene expression and DNA synthesis. Methylcobalamin which serves as a cofactor in the methylation cycle, is involved in the production of methionine from homocysteine by the action of MTHFR. Low dietary intake of either or both folate and vitamin B12 will result in low methionine levels, which would ultimately inhibit the formation of homocysteine.
MTHFR Basics: Diet and Supplement Strategies for People with MTHFR
MTHFR deficiency may also lead to low homocysteine levels in the body. MTHFR is the enzyme responsible for the transfer of a methyl group from N5,N10-methylenetetrahydrofolate to homocysteine forming methionine. Defects in the gene, most notably the C677T gene polymorphism, may result in low 5-MTHF levels, resulting in hypohomocysteinemia.5
The effects of having hypohomocysteinemia are mainly due to the prolonged depletion of cysteine. That said, the effects of hypohomocysteinemia would be the prolonged inflammatory insults experienced by the body due to the increased formation of free radicals with the lack of GSH to counteract the effect. Inflammation can lead to several disorders that may affect the cardiovascular system, nervous system, and even the renal system. Atherosclerosis is a major concern due to the inflammatory nature of the disease. Inflammation will induce the misfolding of the proteins in the brain causing Alzheimer’s disease. Chronic renal failure may result in the increased inflammation of the tubular system. GSH plays a central role in mediating the effects of oxidative stress, preventing damage to the organs. That said, GSH production relies heavily on the pool of homocysteine to fuel its synthesis.
Check this Comprehensive info on what homocysteine is and why it’s tested, including metabolism and clinical use.
What Does Low Homocysteine Mean?
Understanding homocysteine’s role in your body:
Homocysteine is an amino acid that sits at a critical crossroads in your body’s biochemistry. It’s not just a waste product to be eliminated — it’s an important intermediate compound that your body uses to create essential substances:
- Glutathione (GSH) — your body’s master antioxidant that protects cells from oxidative damage
- SAMe (S-adenosylmethionine) — your universal methyl donor needed for hundreds of reactions
- Cysteine — a building block for proteins and antioxidants
- Methionine — an essential amino acid needed for protein synthesis
Think of homocysteine as a busy intersection where traffic flows in multiple directions. When homocysteine levels are too low, it suggests that traffic is being diverted heavily in one direction, potentially leaving other pathways undersupplied.
What causes low homocysteine levels?
Several factors can drive homocysteine levels down below normal:
-
Increased demand for glutathione production
When your body is under oxidative stress — from toxins, inflammation, infections, or chronic illness — it prioritizes making glutathione to combat free radicals. This pulls homocysteine down the transsulfuration pathway to produce cysteine, which is then used to make glutathione.
Low homocysteine may actually be a sign your body is fighting oxidative stress , not a sign of good health.
-
Increased detoxification demands
Your liver uses sulfation (a Phase II detoxification pathway) to eliminate toxins, medications, and hormones. This process requires cysteine, which comes from homocysteine. Heavy detoxification loads can deplete homocysteine as it’s converted to cysteine to support sulfation.
MTHFR and Methylation in Clinical Practice
Common triggers include:
- Alcohol consumption
- Medication use
- Environmental toxin exposure
- High-fat diet (requires taurine production from cysteine)
- Hormone metabolism (estrogen detoxification)
-
Low protein intake
Homocysteine is created from methionine, an essential amino acid found primarily in animal proteins (meat, fish, eggs, dairy). If you don’t consume enough protein, or follow a vegan/vegetarian diet without adequate plant-based protein sources, you may not have enough methionine to maintain normal homocysteine levels.
-
Vitamin B deficiencies
Paradoxically, deficiencies in folate and vitamin B12 can cause low homocysteine because these vitamins are needed to recycle homocysteine back into methionine. Without adequate B vitamins, your body can’t produce enough homocysteine in the first place.
-
MTHFR gene mutations
Certain MTHFR variants can reduce the enzyme’s activity so much that homocysteine can’t be efficiently recycled into methionine, potentially leading to lower baseline homocysteine levels in some individuals, particularly when combined with low B-vitamin intake.
-
CBS gene mutations
The CBS (cystathionine beta-synthase) gene controls the enzyme that converts homocysteine into cysteine. Some CBS variants cause the enzyme to work too quickly, rapidly depleting homocysteine by shunting it down the transsulfuration pathway.
What low homocysteine tells you:
Low homocysteine levels can indicate:
- Active oxidative stress — your body is using homocysteine to make antioxidants
- Heavy detoxification burden — liver is working overtime to eliminate toxins
- Inadequate protein intake — not enough methionine coming from diet
- Vitamin B deficiencies — despite what you might expect
- Chronic inflammation — ongoing immune activation
- Metabolic imbalances — issues with methylation or transsulfuration pathways
The clinical picture matters:
Low homocysteine isn’t automatically problematic. Context is everything:
- If you’re healthy with no symptoms — low-normal homocysteine may be fine
- If you have chronic illness, fatigue, or inflammation — low homocysteine may indicate your body is under stress
- If you’re vegan/vegetarian with low protein intake — may simply need more dietary methionine
- If you have multiple chemical sensitivities — may indicate overtaxed detoxification pathways
The key question isn’t just “Is my homocysteine low?” but rather “Why is my homocysteine low, and what does it mean for my overall health?”
Trusted academic medical center info on normal ranges, functions, and implications of homocysteine levels.
Low Homocysteine vs High Homocysteine
Both low and high homocysteine levels can indicate health problems, but they tell very different stories about what’s happening in your body. Understanding the distinction helps you and your healthcare provider determine the right approach.
High Homocysteine (Hyperhomocysteinemia)
What it means: Homocysteine is building up in your blood because your body can’t efficiently convert it into other useful compounds. It’s like a traffic jam at that critical biochemical intersection.
Common causes:
- MTHFR gene mutations (C677T, A1298C) reducing enzyme efficiency
- Vitamin B deficiencies (folate, B12, B6) preventing homocysteine recycling
- Kidney disease impairing homocysteine clearance
- Certain medications (methotrexate, antacids, metformin)
- Hypothyroidism
- Aging
Health risks associated with high homocysteine:
- Cardiovascular disease — damages blood vessel walls, promotes atherosclerosis
- Blood clots — increases risk of DVT, pulmonary embolism, stroke
- Heart attack and stroke — particularly when levels exceed 15 μmol/L
- Pregnancy complications — miscarriage, preeclampsia, neural tube defects
- Cognitive decline — Alzheimer’s disease, dementia, memory problems
- Osteoporosis — weakens bone structure
- Depression and mental health issues
Treatment approach:
- Increase methylated B vitamins (methylfolate, methyl-B12, B6)
- Improve diet with folate-rich foods
- Address underlying deficiencies
- Support methylation pathways
- Monitor and reduce levels to optimal range (below 10 μmol/L)
The goal: Lower homocysteine by improving your body’s ability to process it efficiently.
Low Homocysteine (Hypohomocysteinemia)
What it means: Homocysteine is being used up too quickly or not being produced in sufficient amounts. Your body is pulling heavily from the homocysteine pool to meet other urgent demands, or you’re not creating enough in the first place.
Common causes:
- Oxidative stress demanding increased glutathione production
- Heavy detoxification burden (toxins, alcohol, medications)
- Low protein/methionine intake (especially in vegans/vegetarians)
- CBS gene mutations causing rapid conversion to cysteine
- Paradoxically, severe B-vitamin deficiencies
- Chronic inflammation or infection
- Malnutrition or eating disorders
Health concerns associated with low homocysteine:
- Oxidative stress — insufficient antioxidant reserves despite high demand
- Chronic inflammation — ongoing immune activation and tissue damage
- Protein deficiency — inadequate amino acid intake
- Impaired methylation — not enough homocysteine to recycle into SAMe
- Detoxification overload — liver working overtime
- Cardiovascular issues — yes, even low homocysteine can contribute to atherosclerosis through different mechanisms
- Muscle wasting — in severe cases with malnutrition
- Neurological problems — from chronic oxidative damage
Treatment approach:
- Increase protein intake, especially methionine-rich foods
- Address underlying oxidative stress and inflammation
- Support glutathione production directly (NAC, glycine, glutamine)
- Reduce toxic burden and support detoxification
- Address root causes (infections, mold, chronic illness)
- May need to temporarily avoid high-dose methylated B vitamins
The goal: Address why homocysteine is being depleted rather than simply trying to raise levels.
The optimal range:
Most functional medicine practitioners consider optimal homocysteine levels to be:
- 7-8 μmol/L — ideal range for most people
- Below 6 μmol/L — may warrant investigation, especially with symptoms
- Above 10 μmol/L — increased cardiovascular risk
- Above 15 μmol/L — significantly elevated, requires intervention
Why both extremes matter:
The medical community has focused heavily on high homocysteine for decades because the cardiovascular risks are well-established. However, low homocysteine is increasingly recognized as a marker of:
- Chronic oxidative stress
- Metabolic dysfunction
- Nutritional inadequacy
- Overtaxed detoxification systems
Neither extreme is ideal. Your body needs homocysteine in the right amount — enough to support methylation and protein synthesis, but not so much that it accumulates and causes vascular damage.
Clinical approach:
When interpreting homocysteine levels, consider:
- Your symptoms — fatigue, inflammation, cardiovascular issues?
- Your diet — adequate protein and B vitamins?
- Your genetics — MTHFR, CBS, or other methylation variants?
- Your toxic burden — exposure to mold, chemicals, medications?
- Your overall health — chronic illness, infections, stress levels?
Both high and low homocysteine require investigation, but the treatment approaches are fundamentally different. This is why working with a knowledgeable practitioner who understands the nuances of homocysteine metabolism is essential for proper management.
Frequently Asked Questions About Low Homocysteine
1. What is considered a low homocysteine level?
Homocysteine levels are measured in micromoles per liter (μmol/L) through a simple blood test. What’s considered “low” can vary slightly between laboratories and practitioners, but general guidelines are:
Standard reference ranges:
- Normal range: 5-15 μmol/L (though this is quite broad)
- Low homocysteine: Below 5 μmol/L
- Very low homocysteine: Below 3-4 μmol/L
Functional medicine optimal ranges:
Many integrative and functional medicine practitioners use tighter ranges:
- Optimal: 6-9 μmol/L
- Low-normal: 5-6 μmol/L (may be fine if asymptomatic)
- Low: Below 5 μmol/L (warrants investigation)
- Concerning: Below 3 μmol/L (definitely needs evaluation)
Context matters:
Whether your homocysteine level is “too low” depends on several factors:
You may be fine with low-normal levels (5-6 μmol/L) if:
- You have no symptoms
- You eat adequate protein
- Your B-vitamin levels are good
- You have no chronic health issues
- You feel energetic and healthy
Low levels (below 5 μmol/L) may be concerning if:
- You have chronic fatigue or low energy
- You experience frequent infections or poor immunity
- You have signs of oxidative stress (inflammation, pain, skin issues)
- You’re dealing with chronic illness
- You have multiple chemical sensitivities
- You follow a very low protein or vegan diet
- You have unexplained symptoms
Age and gender considerations:
Homocysteine levels naturally vary by:
- Age — tends to increase slightly with age
- Gender — men typically have slightly higher levels than women
- Pregnancy — levels often drop during pregnancy (this is normal)
- Menopause — levels may increase after menopause
When to test:
Homocysteine testing is typically done:
- Fasting (8-12 hours without food) for most accurate results
- In the morning when possible
- Before starting B-vitamin supplementation (if you want baseline levels)
- Alongside B12, folate, and other relevant markers
The bottom line: Homocysteine below 5 μmol/L is generally considered low, and levels below 3-4 μmol/L warrant investigation, especially if you have symptoms. However, the number alone doesn’t tell the whole story — your symptoms, diet, health history, and other lab markers provide essential context for interpretation.
Can low homocysteine be dangerous?
Yes, low homocysteine can potentially be dangerous, though it’s often overlooked compared to the well-known risks of high homocysteine. The dangers depend on why your homocysteine is low and what’s happening in your body as a result.
Direct health risks of low homocysteine:
-
Indicator of chronic oxidative stress
Low homocysteine often signals that your body is under significant oxidative stress and is rapidly converting homocysteine to cysteine to produce glutathione (your master antioxidant). This suggests:
- Ongoing cellular damage from free radicals
- Increased inflammation throughout the body
- Accelerated aging at the cellular level
- Higher risk of chronic diseases
The danger: You’re fighting a losing battle against oxidative damage, which can lead to cardiovascular disease, neurological decline, cancer, and autoimmune conditions.
-
Impaired methylation capacity
When homocysteine is too low, you may not have enough available to recycle back into methionine and SAMe (your universal methyl donor). This can impair:
- DNA repair and gene expression
- Neurotransmitter production (serotonin, dopamine)
- Hormone metabolism and detoxification
- Immune system function
- Energy production
The danger: Poor methylation affects virtually every system in your body, contributing to mood disorders, hormonal imbalances, fatigue, and increased disease risk.
-
Protein and amino acid deficiency
Very low homocysteine may indicate inadequate protein intake or malnutrition, particularly lack of methionine (found mainly in animal proteins). This can cause:
- Muscle wasting and weakness
- Poor wound healing
- Compromised immune function
- Hair loss and brittle nails
- Fatigue and low energy
The danger: Chronic protein deficiency leads to malnutrition-inflammation-cachexia syndrome, particularly concerning in elderly individuals or those with chronic kidney disease.
-
Cardiovascular disease progression
Surprisingly, both high AND low homocysteine have been associated with cardiovascular disease, though through different mechanisms:
- High homocysteine directly damages blood vessels
- Low homocysteine may indicate chronic inflammation and oxidative stress that also promote atherosclerosis
The danger: You can still develop heart disease even with low homocysteine if the underlying oxidative stress and inflammation aren’t addressed.
-
Detoxification overload
Low homocysteine may signal that your liver is working overtime to detoxify substances through sulfation pathways, depleting your homocysteine pool. This can indicate:
- Toxic burden from environmental chemicals, mold, or medications
- Impaired liver function
- Hormonal imbalances from poor estrogen clearance
The danger: Chronic detoxification stress exhausts your body’s resources and can lead to multiple chemical sensitivities, hormonal disorders, and liver dysfunction.
When low homocysteine is most dangerous:
Low homocysteine is particularly concerning when combined with:
- Chronic illness — autoimmune disease, cancer, chronic infections
- Severe symptoms — debilitating fatigue, cognitive decline, chronic pain
- Malnutrition — eating disorders, severe dietary restriction, elderly with poor appetite
- Kidney disease — where low homocysteine predicts worse outcomes
- Multiple chemical sensitivities — indicating overtaxed detoxification
- Very low levels — below 3-4 μmol/L
When low homocysteine is less concerning:
You’re probably fine if:
- You’re healthy and asymptomatic
- Your levels are low-normal (5-6 μmol/L) rather than very low
- You eat adequate protein and have good B-vitamin status
- You have no signs of oxidative stress or inflammation
- Your other lab markers are normal
Here is Professional laboratory test catalog explaining homocysteine metabolism and clinical significance.
The bottom line: Low homocysteine can be dangerous when it reflects underlying oxidative stress, chronic inflammation, malnutrition, or metabolic dysfunction. It’s not the low number itself that’s dangerous — it’s what the low number is telling you about your body’s state. If you have low homocysteine along with symptoms or chronic health issues, it deserves investigation and treatment of the root causes.
Should you supplement if homocysteine is low?
The answer depends on why your homocysteine is low and what other factors are at play. Unlike high homocysteine (where the treatment is usually straightforward — add methylated B vitamins), low homocysteine requires a more nuanced approach.
-
If you have signs of methyl overload or overmethylation:
Some people with low homocysteine actually have too much methylation activity or can’t utilize methyl groups properly. Adding more methylated B vitamins can make things worse.
Signs you might have methyl overload:
- Anxiety, agitation, or feeling “wired” on methylated supplements
- Insomnia or racing thoughts
- Irritability or mood swings
- Rapid heartbeat or palpitations
- Headaches or migraines triggered by methylfolate or methyl-B12
What to do instead: Focus on addressing blockages preventing methyl utilization (gut health, infections, toxins) rather than adding more methyls.
-
If low homocysteine is from CBS upregulation:
If you have CBS gene mutations causing rapid conversion of homocysteine to cysteine, adding methylated B vitamins may further lower homocysteine without addressing the underlying issue.
What to do instead: Support the transsulfuration pathway with molybdenum, consider limiting high-sulfur foods temporarily, and address why CBS is overactive.
-
If you’re under significant oxidative stress:
When low homocysteine reflects your body desperately making glutathione to fight oxidative damage, adding methyl donors might not help and could potentially increase oxidative stress.
What to do instead: Support glutathione production directly and address sources of oxidative stress first.
When supplementation MAY be helpful:
-
If low homocysteine is from inadequate protein/methionine intake:
If you’re vegan, vegetarian, or eating very low protein, your body simply doesn’t have enough raw materials to make homocysteine.
What to supplement:
- Increase dietary protein first (see foods section below)
- Consider methionine supplements (500-1000mg daily) under practitioner guidance
- May benefit from small amounts of methylated B vitamins once protein intake is adequate
-
If you have B-vitamin deficiencies:
Paradoxically, severe B12 or folate deficiency can cause low homocysteine because you can’t recycle it properly.
What to supplement:
- Start with low doses of methylated B vitamins (e.g., 400-800mcg methylfolate, 500-1000mcg methyl-B12)
- Increase gradually while monitoring symptoms
- Include B6 and other B-complex vitamins
- Retest homocysteine after 2-3 months
-
If low homocysteine is accompanied by low SAMe:
If testing shows both low homocysteine and low SAMe, you may benefit from methylation support.
What to supplement:
- Methylated B vitamins at moderate doses
- SAMe supplements under supervision
- Trimethylglycine (TMG/betaine) to support methylation
Supplements that may help regardless of cause:
For oxidative stress and glutathione support:
- NAC (N-acetylcysteine): provides cysteine directly
- Glycine: another glutathione building block
- Glutamine: supports gut health and glutathione
- Vitamin C: antioxidant support
- Alpha-lipoic acid: regenerates glutathione
- Selenium: supports glutathione peroxidase
The careful approach to supplementation:
Step 1: Identify the root cause
- Test B12, folate, and other relevant markers
- Assess diet and protein intake
- Consider genetic testing (MTHFR, CBS, COMT)
- Evaluate for oxidative stress, inflammation, or toxic burden
Step 2: Address foundations first
- Optimise diet (see foods section)
- Reduce toxic exposures
- Support gut health
- Manage stress
- Improve sleep
Step 3: Start low and go slow
- Begin with lowest effective doses
- Introduce one supplement at a time
- Monitor symptoms carefully
- Adjust based on response
Step 4: Retest and reassess
- Recheck homocysteine after 2-3 months
- Monitor symptoms and overall health
- Adjust supplementation accordingly
Work with a knowledgeable practitioner:
Low homocysteine is complex and requires individualised treatment. A practitioner experienced in methylation, functional medicine, or integrative health can:
- Interpret your labs in context
- Identify root causes
- Design appropriate supplement protocols
- Monitor your progress
- Adjust treatment as needed
The bottom line: Don’t automatically supplement with methylated B vitamins if your homocysteine is low. First, determine why it’s low. If it’s from inadequate protein or B-vitamin deficiency, supplementation may help. If it’s from oxidative stress, CBS upregulation, or methyl overload, supplementation could worsen the problem. Focus on addressing root causes and supporting your body’s specific needs rather than blindly trying to raise the number.
What foods increase homocysteine naturally?
If you have low homocysteine due to inadequate protein or methionine intake, increasing specific foods can help raise levels naturally. The key is consuming foods rich in methionine — the essential amino acid that your body converts into homocysteine.
Highest methionine-rich foods (animal sources):
- Meat and poultry
- Fish and seafood
- -Eggs and dairy:
Practical serving sizes:
To put this in perspective, here’s how much methionine you’d get from typical servings:
- 150g chicken breast: ~1,400mg methionine
- 100g tuna steak: ~1,100mg methionine
- 2 large eggs: ~380mg methionine
- 200g Greek yogurt: ~560mg methionine
- 30g Parmesan cheese: ~360mg methionine
Plant-based methionine sources:
For vegetarians and vegans, getting adequate methionine requires more planning:
- Nuts and seeds
- Legumes
- Grains
How much methionine do you need?
Recommended daily intake:
- Adults: 10-13mg per kg body weight per day
- For a 70kg (154lb) person: approximately 700-910mg methionine daily
- Athletes or those with higher needs: 15-20mg per kg body weight
Sample daily meal plan to increase homocysteine:
Breakfast:
- 2 eggs scrambled (380mg)
- 30g cheese (200mg)
- Total: ~580mg methionine
Lunch:
- 150g chicken breast (1,400mg)
- Quinoa salad (95mg per 100g serving)
- Total: ~1,500mg methionine
Snack:
- 30g Brazil nuts (300mg)
- Total: ~300mg methionine
Dinner:
- 150g salmon (940mg)
- Roasted vegetables
- Total: ~940mg methionine
Daily total: ~3,320mg methionine (well above minimum requirements)
Vegan/vegetarian meal plan:
Breakfast:
- Oatmeal with hemp seeds and Brazil nuts (500mg+)
- Fortified plant milk (varies)
Lunch:
- Tofu stir-fry with quinoa (400mg+)
- Sesame seed garnish (100mg)
Snack:
- Sunflower seed butter on whole grain bread (300mg)
Dinner:
- Lentil and chickpea curry (200mg)
- Brown rice (60mg)
Daily total: ~1,560mg methionine (adequate for most people, though lower than omnivorous diet)
Important considerations:
- Balance is key: You want to raise homocysteine to optimal levels (6-9 μmol/L), not create high homocysteine. Monitor with blood tests.
- Include B vitamins: Eating methionine-rich foods without adequate B vitamins could potentially raise homocysteine too high. Ensure balanced nutrition.
- Quality matters: Choose high-quality protein sources:
- Grass-fed beef
- Wild-caught fish
- Pasture-raised eggs and poultry
- Organic dairy when possible
- Vegetarians/vegans need to be strategic: Combine multiple plant protein sources throughout the day to get adequate methionine.
The bottom line: To naturally increase homocysteine, focus on methionine-rich foods like meat, fish, eggs, cheese, and Brazil nuts. Vegetarians and vegans should emphasize nuts, seeds, legumes, and whole grains while ensuring adequate B-vitamin intake. Aim for balanced nutrition that provides sufficient methionine along with the cofactors needed for healthy homocysteine metabolism, and monitor levels with blood testing to ensure you reach optimal range without overshooting.
REFERENCES:
- Ganguly, P. & Alam, S.F. Role of homocysteine in the development of cardiovascular disease. USA: Nutrition Journal. January 2015; Vol. 14, No. 6.
- Lord, R. & Fitzgerald, K. Significance of Low Plasma Homocysteine. USA: Metametrix Laboratory Department of Science and Education. 2006. Retrieved
- Blom, H. & Smulders, Y. Overview of homocysteine and folate metabolism. With special references to cardiovascular disease and neural tube defects. USA: Journal of Inherited Metabolic Disorders. February 2011; Vol. 34, No. 1. pp. 75-81.
- O’Leary, F. & Samman, S. Vitamin B12 in Health and Disease. USA: Nutrients. March 2010; Vol. 2, No. 3. pp. 299-316.
- Leclerc, D. et al. Molecular Biology of Methylenetetrahydrofolate Reductase (MTHFR) and Overview of Mutations/Polymorphisms. Madame Curie Bioscience Database.